Search Articles
clear search termsHomocysteine: The Hidden Risk Factor Many Doctors Miss
I want you to be aware of one of the most commonly overlooked risk factors in cardiovascular disease (CD). It might save your client’s life. And no, it’s not cholesterol! Modern medical media is overflowing with misguided warnings about cholesterol. We do some heavy-duty myth-busting about cholesterol in our Cardiovascular course. Do you know? Patients in the hospital having had a heart attack are just as likely to have low-normal cholesterol as they are to have elevated cholesterol. Furthermore, people with low cholesterol end up with just as much atherosclerotic plaque in their arteries as those with high cholesterol. And no, LDL is not necessarily the “bad” cholesterol either. What science has proven is not necessarily what you find in news headlines or pharmaceutical advertisements (or internet blog articles either). The truth is often lost in generalization. Myths abound!
The primary driver for CD in most people is inflammation. One of the most common causes of that inflammation is elevated blood sugar. This is why those with insulin resistance (or its progression to Type 2 diabetes) are many times more likely to develop CD than those without. Elevated blood sugar inflames arteries. And the immune system tries to respond to protect and repair the precious arterial lining (also called the endothelium). It is then this out-of-control immune response that leads to progressive build-up of cholesterol, macrophages, and clotting agents in “gunk” that can eventually block an artery and cause a heart attack or stroke. This is atherosclerosis.
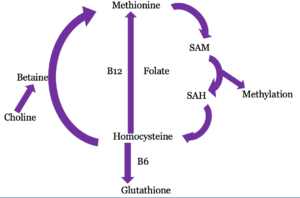 But here’s what you may not know… A major source of inflammation that physicians very seldom assess in those at risk of CD is a marker called homocysteine (often abbreviated HCY on labwork). Homcysteine is an amino acid that the body produces in a biochemical process called methylation. In this process, the body converts the amino acid methionine into homcysteine and back again repeatedly. This ongoing cycle has two particularly powerful outcomes: generating methyl groups (especially for cellular repair such as DNA damage) and making glutathione (the body’s most powerful antioxidant). If this is a new concept to you, don’t let the unfamiliar words be intimidating; you can absolutely understand this material. You may learn more about methylation here and here (it’s a critical process for many body processes such as detoxification too).
But here’s what you may not know… A major source of inflammation that physicians very seldom assess in those at risk of CD is a marker called homocysteine (often abbreviated HCY on labwork). Homcysteine is an amino acid that the body produces in a biochemical process called methylation. In this process, the body converts the amino acid methionine into homcysteine and back again repeatedly. This ongoing cycle has two particularly powerful outcomes: generating methyl groups (especially for cellular repair such as DNA damage) and making glutathione (the body’s most powerful antioxidant). If this is a new concept to you, don’t let the unfamiliar words be intimidating; you can absolutely understand this material. You may learn more about methylation here and here (it’s a critical process for many body processes such as detoxification too).
We generate and need some homocysteine. But like most things in the body, more is not better, and balance is the goal. All by itself, too much homocysteine in the blood can trigger a potentially artery-clogging inflammatory reaction along the endothelium lining. Even moderately elevated homocysteine increases the risk of atherosclerosis. It is an independent risk factor for CD, yet conventional physicians don’t routinely check it! Our clients can have a false sense of security from being told by their physicians that their cholesterol and blood pressure are “fine” and still be at high risk of developing angina, atherosclerosis, or even an imminent heart attack if their homocysteine is chronically elevated (especially those with other risk factors such as insulin resistance or a history of smoking).
What causes the methylation cycle to break down? Why does homocysteine get elevated? Most often because the body lacks sufficient vitamin cofactors to keep the methylation cycle running smoothly, especially the B vitamins B6, B12, and B9 (folate). Sometimes this is due to a nutrient-poor diet (e.g. junk-food-atarian). Other times it is because of impaired nutrient digestion/absorption in the gastrointestinal tract. Many of those who use proton pump inhibitor (PPI) medications for acid reflux end up with insufficient Vitamin B12 due to low stomach acid. Also, gut microbial imbalances (which are common given widespread, frequent antibiotic use) can impair nutrient absorption in the intestines. A substantial portion of the population also has a genetic variant in the methylation cycle called MTHFR which requires extremely high levels of folate in order to methylate efficiently.
The bottom line is that our clients with a family history of CD (or other key risk factors) should have their homocysteine checked (a simple blood test available at any conventional lab). And if it’s significantly elevated above optimal (ideal is typically in the 6-8 nmol/mL range), a high-quality B-vitamin supplements can reduce homocysteine aggressively. As you can easily see in the diagram above, the methylation cycle simply won’t work without these nutrients. To ensure bio-availability to cells, I recommend a supplement that includes the methylcobalamin form of Vitamin B12 and actual folate (not folic acid). Great examples include Metagenics “Vessel Care”, Pure Encapsulations “Homocysteine Factors”, and Xymogen’s “Methyl Protect”. In fact, the B vitamins that help reduce homocysteine are also vital for helping the body to withstand chronic stress and to process a wide array of toxins (other key CD risk factors). I recommend always starting a B-complex supplement in a “half cap” dose (discard half the contents and reassemble the capsule) for at least the five several days – to ensure it is well tolerated. Some people do not well tolerate B-complex supplements, and others simply need a “low’n’slow” introduction to nutrients they have been lacking for quite a while.
Note that a homocysteine level like 12.2 nmol/mL may still be within “typical reference range” for most labs, but keep in mind always that lab reference ranges are not healthy ranges, rather actual data on what the average American presents. Don’t make the mistake of using reference ranges to gauge if a client labwork marker is healthy.
Of course, elevated homocysteine is seldom the only CD risk factor that our clients need help identifying and addressing. Absolutely, our clients still need help reducing other key inflammation drivers, especially elevated fasting blood sugar (anything above 85 mg/dl is correlated in clinical study with an increased risk of CD for men – again, despite the typical reference range), smoking, hypertension (often insufficient potassium is a key driver), insufficient sleep, and chronic stress (epidemic, as we know). But knowing a bit more about the body’s biochemistry and simple solutions to common problems can allow you to make even greater contributions to your clients’ and patients’ well-being!
P.S. If you are passionate about transforming healthcare through the power of functional medicine, we encourage you to learn more about SAFM’s practitioner training programs. Enrollment for our next cohort is now open!
To receive weekly clinical tips for practitioners – like this one – right to your inbox, register here.
Follow us on Facebook and/or on Youtube to gain more rich clinical content.
13 Questions for “Homocysteine: The Hidden Risk Factor Many Doctors Miss”
-
7
-
7.1
Physiologically elevated serum B12 levels are rare. We would recommend a triple check of the supplements and any non-supplement powders and anything where there is a potential for added nutrients. Those can lurk also in many food products, simply added as a bonus that can lead to overconsumption. If none of that is present, it would make sense to repeat the serum vitamin B12 test, as lab testing mistakes do happen. Only if high B12 results have been obtained multiple times over a period of time (6 to 12 months) would we recommend digging into physiological reasons for elevated B12 levels which could be associated with liver metabolism issues or solid tumors.
-
-
6
Megan Taylor says:
How long should a client typically be on a Homocysteine supplement? How often do you recheck it once they are on a supplement?
-
6.1
Checking the homocysteine levels every 3-6 months after the start of supplementation is a good time interval. The length of time for how long it is needed will depend greatly on why the homocysteine is high in the first place.
-
-
5
Marie Campins says:
What about hyperhomocysteinemia that doesn’t lower even with B Complex, could there be some GUT issues of B12 absorption?
-
5.1
SAFM Team says:
Certainly. In the same vein, the old adage, “You are what you eat” is woefully over-simplified, we must be able to digest, absorb, convert to final forms, and get past the cell membrane the nutrients that we need to run our biochemistry. This is true whether the source be food or supplement! Many factors could be at play including, for example, impaired intestinal absorption of Vitamin B12 (e.g. due to metformin drug use) or poor conversion of the typical pyridoxine form of Vitamin B6 (found is most B-complex supplements) to the activated pyridoxal-5-phosphate form. Genetic dynamics could also be at play, such as MTR or MTRR variants causing poor utilization and retention of B12 or MTHFR variants causing poor availability of folate in the methylation cycle (which is often helped with ensuring ample intake of riboflavin, Vitamin B2); these may necessitate notably higher doses than others require for modulation of homocysteine.
-
-
4
Carolyne Shapiro says:
Great information and thank you so much!! It is indeed interesting how little Homocysteine is tested for and yet how often we are told that an elevated LDL — even by like 6 points warrants use of a statin.
-
3
Great article Tracy, thank you. So simple and understandable, and so full of pearls. You recommend starting a B-complex supplement in a “half cap” dose in a way that clients discard half the content and reassemble the capsule. This wonderful supplements are pretty expensive in my country (Croatia) and I have a hard time convincing clients first to consider them and then to buy them. Do you see any problem with using empty cellulose capsule and just fill it with the half of B vit powder instead of throwing it, so 1 cap can be used for 2 days? Just being practical 🙂
-
3.1
We see no problem at all with your solution, Ana. Being practical may mean for some clients filling up cellulose or a veggie capsule to ensure the usage of every last ounce of the supplement, and for others, it will be saving time by discarding 1/2 of the first 3-5 doses and getting on with their lives. It’s a personal choice.
-
-
2
There is a lot of info about elevated homocysteine being bad. But, can suboptimal homocysteine be an indicator of poor methylation? Could this mean that there may not be enough SAM-e or methionine which are needed for the other parts of the Methylation cycle?
-
2.1
Indeed there are quite a few papers on elevated homocysteine (HCY), especially in connection to cardiovascular disease, and somewhat surprisingly little clinical study on the impact of low homocysteine, so alas, we don’t have much to offer you there. In principle, low HCY would present less of an opportunity to make glutathione, so there could theoretically be a corresponding impact on either oxidative stress or toxicity. What we have seen in practice is that low HCY was associated with an overt issue with either low protein intake or protein maldigestion. Either of these could, of course, reduce the amount of available methionine (especially perhaps in a vegan diet) to drive the methylation process.
-
-
1
The above link is outdated: “You may learn more about methylation here.”
Any other suggestions for methylation explanation?
-
1.1
Good catch – thanks! We’ve fixed the links now with a couple of good options.
-
Ask a Question
Practitioner clarification questions are welcome! Please do not post personal case inquiries.
© 2017-, The School of Applied Functional Medicine | Company Values | Terms of Use | Legal/Privacy | Contact
web development by: Gordon Multimedia
I’m wondering what would cause an elevated B 12 – I have a very healthy pt, eats very clean, no processed foods and only takes Vitamin D who had a Vit B -12 of 2000, she double checked all of her supplements and NONE of them have b vitamins in them. We are puzzled as to what could cause this.